

Pression partielle d'oxygène - pO2
La quantité d'oxygène dans le sang est contrôlée par de nombreuses variables, par exemple la ventilation/perfusion. pO2 est la pression partielle d'oxygène dans une phase gazeuse en équilibre avec le sang. pO2 ne reflète qu'une petite fraction (1 à 2%) de l'oxygène total du sang dissous dans le plasma sanguin [3]. Les 98 à 99% restants de l'oxygène présent dans le sang sont liés à l'hémoglobine des érythrocytes.
pO2 reflète principalement l'absorption d'oxygène dans les poumons.
Intervalle de référence pO2 - exemples
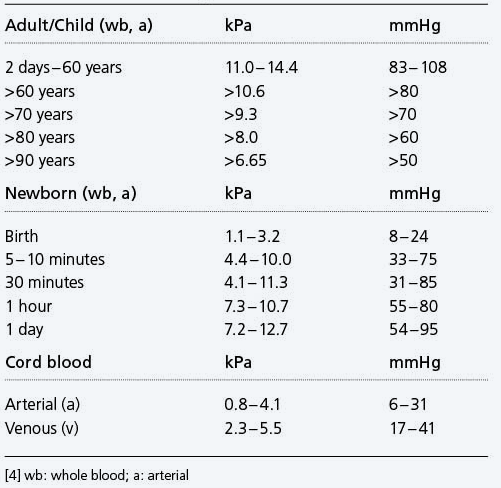
pO2(a) diminue à un rythme de~0,29 kPa (2,2 mmHg) par décennie après l'âge de 40 ans [5].
Signification physiologique de pO2
La vie dépend de l'apport continu d'oxygène aux cellules tissulaires, qui à son tour dépend de l'oxygénation continue du sang veineux dans les poumons. L'oxygène se diffuse vers le bas d'un gradient de pression d'un niveau relativement élevé (21,2 kPa (159 mmHg) au niveau de la mer) dans l'air inspiré, pour abaisser progressivement les niveaux dans les voies respiratoires, le gaz alvéolaire, le sang artériel, les capillaires et enfin la cellule/mitochondries , où le niveau le plus bas pO2 (1 - 1,5 kPa (7,5 - 11,5 mmHg)) est observé. Cette diminution de pO2 entre l'air inspiré et les mitochondries s'appelle la cascade d'oxygène (Fig.3). Le gradient de pression de la cascade d'oxygène est physiologiquement essentiel pour l'apport d'oxygène inspiré aux tissus, et une perturbation pathologique de la cascade, comme celle qui se produit lors de l'hypoventilation, peut entraîner une hypoxie tissulaire [6, 7].

FIG. 3 : La cascade d'oxygène.
Bien que pO2 ne représente qu'une très petite fraction de l'oxygène total (ctO2) (voir ctO2) étant transporté dans le sang artériel, il est très significatif car il est le déterminant majeur de la quantité d'oxygène lié à l'hémoglobine (voir sO2) et donc la quantité totale d'oxygène transportée par le sang artériel et mise à la disposition des cellules tissulaires. La relation entre pO2 et sO2 est décrite par le courbe de dissociation de l'oxyhémoglobine (ODC) (Fig.4). Lorsque pO2(a) est supérieur à 10 - 11 kPa (75 - 83 mmHg), l'hémoglobine se lie à des quantités quasi maximales d'oxygène(c'est-à-dire sO2(a)> 95%). Cependant, si pO2(a) tombe en dessous de∼10 kPa (75 mmHg), il y a une nette diminution de sO2 et donc une forte baisse de la capacité de transport d'oxygène du sang. L'apport d'oxygène aux tissus est de plus en plus compromis lorsque pO2(a) tombe en dessous de∼10 kPa (75 mmHg), non pas principalement parce que pO2(a) est diminué, mais parce que l'hémoglobine transporte beaucoup moins d'oxygène.

FIG. 4 : Courbe de dissociation de l'oxyhémoglobine, y compris les facteurs étrangers déterminant le décalage gauche et droit. Pour plus d'informations sur l'ODC, consultez p50. 2,3-DPG : 2,3-diphosphoglycérate
Pourquoi mesurer la pO2 ?
Le pO2 est le reflet de l'absorption d'oxygène dans les poumons.
- Il s’agit du paramètre clé qui permet d’évaluer la bonne oxygénation du sang, c.-à-d. le transfert de l’oxygène environnemental des poumons (alvéoles) vers le sang (voir statut d’oxygène).
- Il fournit les moyens de diagnostiquer l'insuffisance respiratoire
- Il fournit les moyens de surveiller l'oxygénothérapie supplémentaire
Quand doit-on mesurer la pO2 ?
La mesure de pO2 est cliniquement utile pour le diagnostic, l’évaluation et le suivi des patients atteints d’une maladie respiratoire aiguë ou chronique grave ou d’une insuffisance respiratoire due à des affections autres que maladie respiratoire (par exemple, traumatisme cérébral ou thoracique, surdosage médicamenteux).
Interprétation clinique
Termes utilisés dans l'interprétation
L'hypoxémieest une diminution de la teneur en oxygène (voir ctO2) dans le sang (tableau I). Il existe deux causes principales : une altération de l'oxygénation du sang dans les poumons et une anémie. Le premier est évident comme une diminution de pO2 et le second est évident comme une diminution de l'hémoglobine. Il est important de se rendre compte que, bien que l’hypoxémie est habituellement associée à une diminution de pO2 ,il peut se produisent, par exemple, chez des patients souffrant d’anémie sévère, d’intoxication au monoxyde de carbone et de méthémoglobinémie, malgré un pO2 [8, 9] normal .
L'hypoxie[10] fait référence à l'état potentiellement mortel dans lequel l'apport d'oxygène aux cellules tissulaires n'est pas suffisant pour maintenir un métabolisme aérobie normal. Les cellules tissulaires affectées produisent un excès d'acide lactique, ce qui entraîne une augmentation des taux de lactate dans le sang et une acidose métabolique (voir lactate). Quatre types d'hypoxie sont reconnus; elles sont :
Hypoxie hypoxémique:
Mécanisme d'oxygénation défectueux dans les poumons, entraînant une teneur insuffisante en oxygène dans le sang (ctO2(a) est faible en raison d'un faible pO2(a))
Hypoxie ischémique:
Transport insuffisant d'oxygène vers les tisisus, en raison d'un flux sanguin insuffisant
Hypoxie anémique:
Teneur en oxygène insuffisante dans le sang en raison d'une diminution de la quantité d'hémoglobine capable de transporter l'oxygène
Hypoxie histotoxique:
Mauvaise utilisation de l'oxygène par les tissus
Quel que soit le mécanisme, il peut, s'il est suffisamment sévère, entraîner une anoxie (arrêt de l'apport d'oxygène) et la mort des cellules tissulaires. L'infarctus du myocarde est un exemple d'hypoxie tissulaire locale potentiellement mortelle causée non pas par une hypoxémie, mais par une ischémie, due à une thrombose d'une artère coronaire [11].
L’hyperoxémie est augmentée pO2 dans le sang, c’est-à-dire pO2(a) > 16,0 kPa (120 mmHg) (tableau I). Cela ne peut se produire que dans un cadre clinique avec administration d'oxygène supplémentaire. Cela peut entraîner une hyperoxie (augmentation de la teneur en oxygène dans les tissus). L'hyperoxie peut être associée à la toxicité de l'oxygène; les nouveau-nés prématurés sont particulièrement vulnérables aux effets toxiques de l'oxygène [12].
L'insuffisance respiratoireest l'incapacité des poumons à effectuer correctement les échanges gazeux pulmonaires. Il est défini par pO2(a) <8 kPa (60 mmHg). En dessous du degré d'hypoxémie que représente ce niveau, le risque d'hypoxie augmente, même si le débit cardiaque n'est pas compromis. Ce degré d'hypoxémie déclencherait généralement la prescription d'une thérapie d'oxygène supplémentaire pour assurer une oxygénation adéquate des tissus. (voir CO2 définition de l'insuffisance respiratoire de type I et de type II).

Causes de l'hypoxémie[13]
Symptômes associés à l'hypoxémie[14]
Causes de l'hyperoxémie
Oxygénothérapie et pO2
Trop d'oxygène peut être toxique, provoquant des lésions endothéliales dans les poumons et d'autres tissus. Une augmentation de pO2 ne peut se produire que si la fraction d'oxygène inspiré (FO2(I)) et donc pO2 d'air alvéolaire est augmenté. La seule cause clinique d'augmentation de pO2(a) est l'oxygénothérapie supplémentaire [15].
Au niveau de la mer FO2(I) de l'air ambiant est de 21%. Selon le mode d'administration, l'oxygénothérapie est associée à FO2(I) jusqu'à 100% (oxygène pur). L'oxygénothérapie pose un problème pour interpréter pO2, c'est-à-dire pour décider si le pO2 est suffisamment élevé pour l'augmentation de FO2(I). Une règle empirique utile est que la différence entre FO2(I) (%) et pO2 mesuré en kPa ne doit pas dépasser 10 [16]. Si cette différence est significativement supérieure à 10, l'oxygénation est altérée.
Exemple
Prenons l'exemple de deux patients adultes recevant une oxygénothérapie qui fournit un FO2(I) de 30%. La pO2 (a) du premier patient est de 13 kPa et la pO2(a) du deuxième patient est de 22 kPa. En utilisant la règle empirique, il est clair que le premier patient a une oxygénation altérée malgré la normale pO2 (a). Le deuxième patient ne le fait pas; ce patient pO2 (a) est suffisamment élevé pour l'administration d'oxygène.
Radiometer utilise Microsoft AZURE Active Directory pour fournir un accès sécurisé aux documents, ressources et autres services sur notre portail client pour nos clients et partenaires.
Si votre organisation utilise déjà AZURE AD, vous pouvez utiliser les mêmes identifiants que ceux dont vous vous servez pour accéder au portail client de Radiometer.
Principaux avantages
- Possibilité d'utiliser les identifiants Active Directory existants
- Expérience Single sign-on (authentification unique)
- Utilisation des mêmes identifiants pour accéder à des services futurs
Demander l'accès
Vous recevrez une invitation par e-mail pour accéder à nos services une fois votre demande approuvée.
Une fois que vous acceptez l'invitation, et à condition que votre organisation utilise déjà AZURE AD, vous pouvez utiliser les mêmes identifiants que ceux dont vous vous servez pour accéder au portail client de Radiometer. Sinon, un code secret à usage unique vous sera envoyé par email pour se connecter.